
Most peptide therapy programs cost between $150 and $600 per month once you account for the consultation, the compound itself, and follow-up care. That range is wide because peptides vary a lot in price, and because where you get them, telehealth vs. a physical clinic, changes what you actually spend.
Before you commit to anything, know what you're paying for, what typically gets left off the quoted price, and what insurance will and won't cover. Spoiler on the last one: mostly won't.
What actually drives the price
The single biggest factor is which peptide you're prescribed. Some cost $100 a month to compound. Others hit $400. Brand-name Semaglutide runs over $1,300 a month without insurance. Everything else matters less: who you see, what's bundled, what state you're in.
The second biggest factor is how you access it. Telehealth programs typically run 30–50% cheaper than in-person clinics for the same compound, because clinics carry overhead and often mark up the peptide on top. If both use licensed compounding pharmacies (they should), the peptide quality is the same. You're paying for the delivery model.
One thing people consistently underestimate: lab costs. Most providers require bloodwork before they'll prescribe anything. That typically runs $200–$500 out of pocket and is almost never included in the monthly program fee. Add another round of labs at your 6–8 week check-in and you've added $500–$1,000 to your first year before you've counted a single month's peptide.
Cost by peptide type
These are ranges for pharmaceutical-grade compounds prescribed by a physician and dispensed by a licensed compounding pharmacy.
Growth hormone secretagogues (Sermorelin, Ipamorelin, CJC-1295) $150–$450/month. Sermorelin is usually the cheapest of this group. Ipamorelin and CJC-1295 get prescribed together a lot, and that stack tends to run $250–$450/month.
Healing and recovery peptides (BPC-157, TB-500) $150–$350/month through a compounding pharmacy. You'll see BPC-157 available from research chemical vendors for $25–$50/month, but that's a genuinely different product with no compounding standards, no physician involvement, and no meaningful quality controls.
Anti-aging and skin peptides (GHK-Cu, Epithalon) $150–$400/month. GHK-Cu gets used in both systemic protocols and topical applications.
Immune peptides (Thymosin Alpha-1) $200–$450/month. More expensive than most recovery peptides because the compound is harder to produce.
Semaglutide and GLP-1 agonists This is where the numbers get dramatic. Compounded Semaglutide runs $200–$450/month. Brand-name Wegovy or Ozempic without insurance: $1,000–$1,350/month. Same molecule, very different price. Both require a prescription.
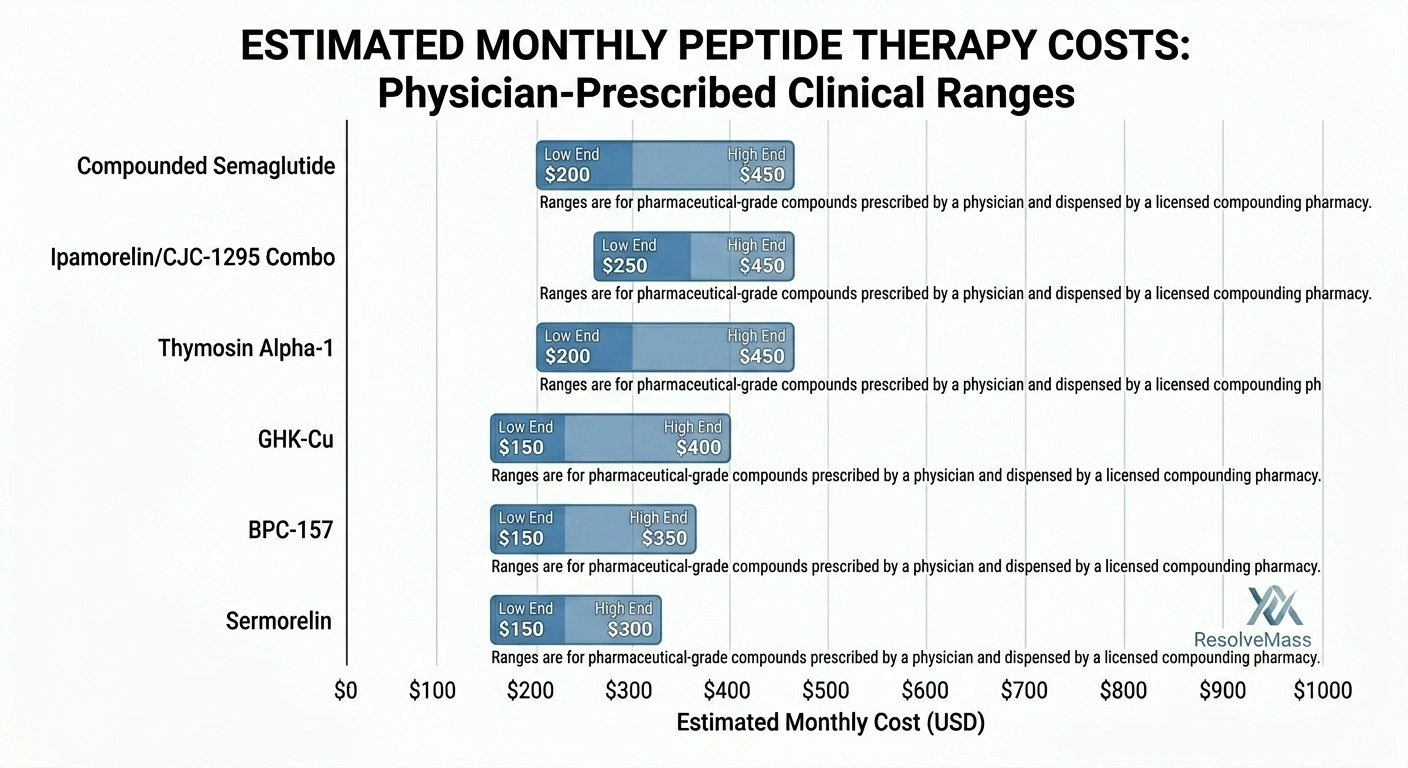
Typical monthly price ranges by peptide category and protocol complexity.
Clinic vs. telehealth
Telehealth has genuinely shifted the cost structure of peptide therapy. A few years ago, you needed a local functional medicine clinic and you paid accordingly. Now most standard protocols can be managed entirely over video.
A telehealth program typically charges $99–$299/month for a single peptide protocol, bundling the consultation, the compound, shipping, and supplies. An in-person clinic charges differently: $200–$500 for the initial consult, $100–$300 per follow-up (usually every 4–12 weeks), and then the peptide cost on top, often with a 30–100% markup over the compounding pharmacy's rate. A single well-run in-clinic protocol can run $500–$1,500/month all in.
Telehealth isn't always the right call. If you're injecting for the first time and want someone to walk you through the process in person, that's a real reason to be in a room with someone. Complex cases with multiple symptoms warrant a more thorough workup. But for a standard single-peptide protocol where your evaluation is mostly based on labs and health history, the lower-cost option delivers comparable clinical quality.
One thing to check: telehealth providers can only prescribe in states where they're licensed. That varies by platform. Worth confirming before you spend time on an intake.
The peptide provider checklist covers what to verify before committing to either option.
What's actually included
The number you see advertised is rarely all-in. Before you agree to anything, ask specifically about each of these.
Most telehealth programs include the physician consultation, the peptide, shipping, and basic supplies (syringes, alcohol swabs, bacteriostatic water if the protocol calls for it). Some fold the initial consultation into the monthly fee; others bill it separately at $150–$300 before your first month starts.
Most programs, telehealth and in-clinic alike, don't include:
- Lab work ($200–$500 per panel)
- Follow-up labs at your 6–8 week check-in
- Visits beyond the base protocol
- Medications for managing side effects
If you build out a realistic first year, it looks something like: initial consultation ($150–$300), two lab panels ($400–$1,000 combined), 12 months of peptide ($150–$450/month), and a couple of follow-up visits ($100–$450). That puts a properly managed first year somewhere between $3,000 and $7,000. Budget programs through telehealth platforms can come in at $1,500–$2,500 if the labs are bundled and you're on a single-peptide protocol.
Insurance
Major US insurers classify peptide therapy as experimental and elective. Aetna, BCBS, UnitedHealthcare: none of them cover it as a baseline. That goes for BPC-157, Ipamorelin, Sermorelin, Thymosin Alpha-1, GHK-Cu, and most of the other peptides people are actually looking for.
GLP-1 agonists are the exception, and only in specific circumstances. Semaglutide prescribed for Type 2 diabetes gets covered by many carriers. Wegovy for weight loss is inconsistent: some state employee plans and Medicare Advantage plans include it, most don't. If Semaglutide is what you're after, call your insurer before assuming anything.
HSA and FSA accounts can be used for peptide therapy paid to a licensed physician — that covers the consultation, lab work, and generally the prescribed compound. You're not getting a discount, but you're spending pretax dollars. Check with your plan administrator, but this is one of the cleaner options most people don't think to ask about.
If you want to try submitting for reimbursement regardless, you'll need itemized receipts, a letter of medical necessity, and ICD-10 codes from your provider. Approval rates are low. Some people get partial reimbursement on labs or consultations even when the peptide itself is denied.
Is this worth spending?
Depends on what you're treating.
GLP-1 agonists: the evidence is there. FDA-approved, extensively studied for weight loss and metabolic outcomes. If you qualify and your insurer covers it (or compounded versions are accessible), the cost-benefit case is as straightforward as it gets in this space.
Growth hormone peptides like Ipamorelin: favorable evidence, but mostly shorter-term. Body composition, sleep, recovery. Genuine outcomes for many people. Long-term data is limited.
Healing peptides like BPC-157: strong animal studies, limited human trials. A lot of physicians prescribe it off-label based on preclinical evidence and what they see in patients. If you need the same quality of evidence you'd expect from a pharmaceutical drug, that evidence doesn't exist yet.
What actually makes any protocol worth the money is whether you approach it correctly. Most peptides need 3–6 months to show meaningful results. Stopping at month three because you haven't noticed a difference doesn't mean the peptide failed. It often just means you didn't give it enough time. That's also the most expensive version of this: spending money on a protocol you abandoned before it could work.
The guide on what peptide therapy actually involves covers what the clinical process looks like by goal. If you want to go deeper on a specific compound, Ipamorelin's profile shows what the per-peptide detail looks like.
Frequently asked questions
Mostly no. Major US insurers classify it as experimental and elective, so you're paying out of pocket for almost everything in this space. The exception is GLP-1 agonists prescribed for Type 2 diabetes: some plans cover that specifically. For anything else, the practical move is to call your insurer and ask about the ICD-10 code your provider is using before you assume the answer either way.
HSA and FSA funds can generally be used here. Peptide therapy paid to a licensed physician as a medical expense qualifies for most people, which lets you spend pretax dollars even when insurance won't cover the cost.
Usually yes, by around 30–50% for the same compound. A telehealth program bundles the consultation, peptide, and shipping into one monthly fee ($99–$299 for most single-peptide protocols). Clinics charge separately for the consult, each follow-up visit, and the peptide itself, often with a markup. The clinical quality is comparable for most standard protocols. The main reasons to go in-person are complexity, preference for hands-on injection training, or a situation that warrants a physical exam.
For legitimate physician-supervised therapy, a single-peptide telehealth program is the entry point, usually $99–$200/month all in. Below that, you're mostly looking at research-grade peptides from unregulated vendors, which is a different product with a different risk profile. The cheapest options you find online often don't involve a physician, a compounding pharmacy, or quality controls of any kind. That's not a cost savings so much as a different category of thing.
Most protocols need at least 3–6 months before you can assess whether they're working. Growth hormone peptides often get cycled: three months on, one month off, or a similar structure. Healing protocols for acute injuries can be shorter. Long-term anti-aging protocols are sometimes used indefinitely, with breaks built in. Your provider should give you a clear timeline at the start, including when you'll review labs and make a real decision about continuing.
Generally yes. Peptide therapy paid to a licensed physician qualifies as a medical expense eligible for HSA/FSA reimbursement, including the consultation, lab work, and typically the prescribed compound. Keep itemized receipts and hold onto the prescription. If your plan administrator pushes back, a letter of medical necessity from your prescribing physician usually resolves it. The rules vary by plan, so it's worth a quick check, but most people find this works.
Published by the PEPVi editorial team. Read our editorial standards.