
Peptides are short chains of amino acids, the same molecules your body uses to build proteins. Your body makes thousands of them right now, and they're running your biology.
If you heard the word on a podcast or saw it trending and want to know what the fuss is about, that's what this covers. "Peptide" turns out to span a much wider range than most people expect: from the active ingredient in your face serum to the drug responsible for most of the weight loss happening in this country right now. That range is the whole story.
The simple definition
An amino acid is a small organic molecule. Your body uses 20 of them as building blocks. String two together and you have a dipeptide. String 10 and you have a decapeptide. Keep adding links, and at some point you've crossed into protein territory.
That line sits around 50 amino acids, though different sources draw it slightly differently. Practically: peptides are small, proteins are large.
Peptides are defined by size and structure, not by function. "Peptide" covers an enormous range: a two-amino-acid food compound and the GLP-1 molecules in Ozempic are both peptides. It's not a drug class. It's not a wellness category. The word describes a molecular shape. What makes any specific peptide interesting or controversial depends entirely on what that peptide does.
Your body produces somewhere between 7,000 and 100,000 distinct peptides. Insulin, oxytocin, and the hunger signal ghrelin are all peptides. Synthetic peptide therapy builds on signals your body already uses.
How peptides differ from proteins
Proteins and peptides are both chains of amino acids, both biological messengers. The difference is size, and size matters more than you'd think.
Larger proteins fold into complex three-dimensional structures. Those shapes determine function, but they also make proteins hard to move around. Getting a full-size protein through a cell membrane is difficult. Getting one to absorb through your skin is nearly impossible.
Peptides move more freely. Short-chain peptides can cross the intestinal lining more readily than proteins, and certain small peptides penetrate skin layers that proteins can't reach. That's one reason peptide skincare formulas tend to outperform ones built on full proteins. The peptide can actually get where it's going.
Smaller chains can also be designed, or found in nature, to fit one specific receptor and trigger one specific response. A protein is like a Swiss army knife. A peptide is like a key cut for one lock.
For a deeper look at the mechanics, how peptides signal cells and trigger biological responses goes into the pathway in detail.
Your body is already full of peptides
Before getting into the injectable compounds, skincare serums, and research chemicals people call synthetic peptides, it's worth knowing that peptides aren't exotic foreign molecules. Your body produces thousands of them, and they're doing essential work right now.
Insulin is a 51-amino-acid peptide. Your pancreas releases it when blood sugar rises, telling cells to absorb glucose. Oxytocin, released during childbirth and social bonding, is a 9-amino-acid peptide. GLP-1, the molecule Ozempic mimics, is a 30-amino-acid peptide your gut releases after meals to signal fullness and kick insulin production into gear.
These aren't edge cases. They're just the famous ones. Peptides:
- Regulate blood pressure and cardiovascular function
- Coordinate immune responses and manage inflammation
- Signal hunger, satiety, and metabolic rate
- Initiate tissue repair after injury
- Carry pain and sensory signals through the nervous system
Hundreds of them are active in your body at any given moment.
When someone talks about peptide therapy, the goal is usually to amplify or mimic a signal the body already sends. Building on a language the body already speaks, not introducing a foreign one. That doesn't make synthetic peptides automatically safe or effective. But it explains the basic logic, and why that logic doesn't always hold up when you push it.
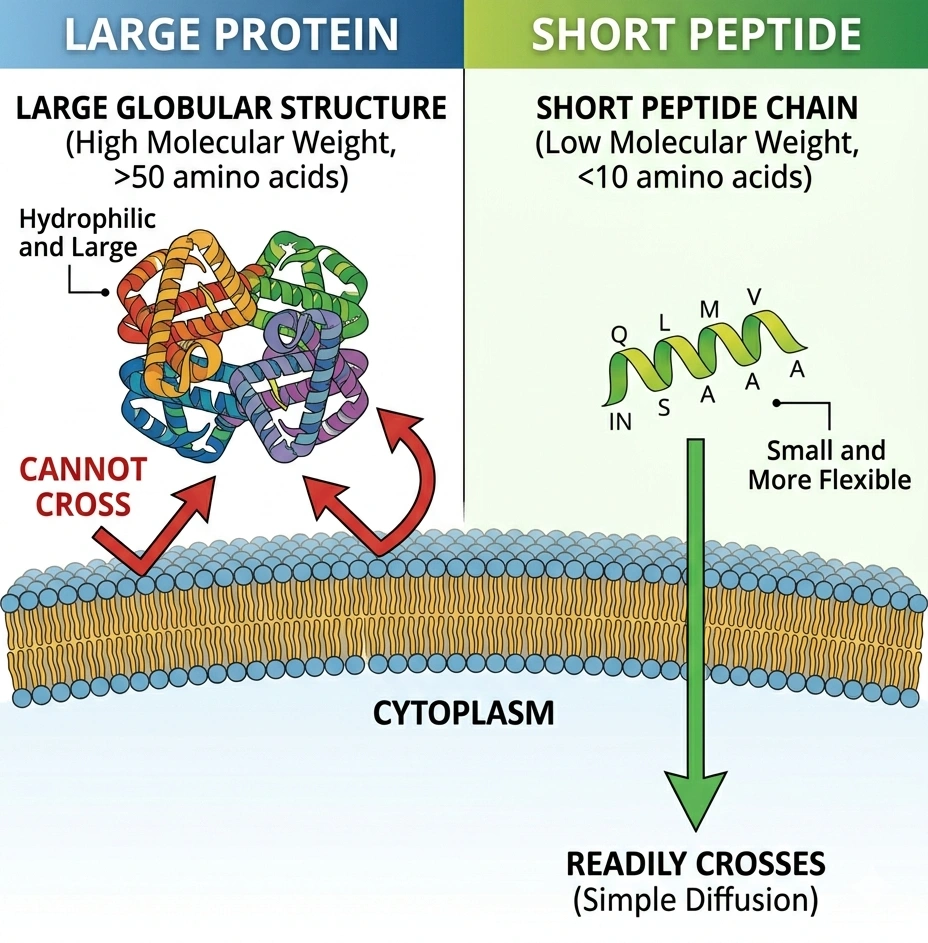
Diagram: large protein vs. short peptide transport across a cell membrane.
How peptides actually work
Peptides do their jobs through receptors — proteins embedded in cell membranes that recognize specific molecules and respond to them.
Think of a cell surface covered in locks. Peptides are the keys. Each lock accepts only the specific key it was built for. When the right peptide binds the right receptor, the receptor changes shape and triggers something inside the cell: a hormone released, a repair process started, an inflammatory signal turned down. Which outcome depends on which receptor and which cell type.
A peptide built to bind the growth hormone secretagogue receptor on the pituitary triggers growth hormone release. It doesn't activate other receptors because it doesn't fit them. In principle, this makes peptides more targeted than older drug classes that hit many different things at once. In principle.
One important problem for anyone hoping to take peptides as pills: most don't survive digestion. Stomach acid and digestive enzymes break peptide bonds, reducing the chain to individual amino acids before it reaches the bloodstream. Those amino acids are nutritious, but they're no longer the specific signal you were trying to send. Clinically meaningful peptide therapies are nearly always injected, sprayed nasally, or applied topically. Delivery method isn't a technicality; it determines whether the peptide can do anything at all. Peptide delivery methods compared covers each route in plain terms.
The three categories worth knowing
When people use the word "peptide," they usually mean one of three different things. They're not equivalent.
Collagen and skincare peptides
Collagen peptides have the most human evidence. These are short chains, often hydrolyzed (partially broken down) for easier absorption, derived from collagen-rich animal sources. Multiple randomized controlled trials have found that oral collagen peptide supplements improve skin elasticity, support joint recovery, and modestly increase bone mineral density.
Oral collagen peptides work differently from the receptor-signaling model. The goal isn't to deliver a specific signal: it's to supply the amino acids (glycine, proline, hydroxyproline) your body uses to build collagen. Even if the peptide chain breaks down in digestion, the raw material still arrives. It's closer to targeted nutrition than to signaling chemistry.
Topical skincare peptides are a different mechanism again. Applied to skin, they skip the digestive system. Certain small peptides, like palmitoyl pentapeptide-4 (the active in Matrixyl) and GHK-Cu, can penetrate the outer skin layer and interact with fibroblasts, the cells that produce collagen. Clinical trials show measurable improvements in fine lines and skin texture for several of these compounds. Effects are modest and vary by formulation, but they're real.
This is the most accessible category. Collagen supplements are at every grocery store. Peptide serums are on every beauty shelf. The evidence base is solid relative to what you'll see in the other two categories, and the risk profile is low.
Therapeutic peptides (FDA-approved drugs)
This is where peptide science has its strongest record: over 80 FDA-approved peptide drugs in clinical use as of 2023, most of which people have encountered without knowing it.
Insulin was the first lab-synthesized peptide, introduced in 1923. GLP-1 receptor agonists (Ozempic, Wegovy, Mounjaro) are peptide drugs with some of the most rigorously tested clinical data of any drug class in recent history. Tesamorelin treats HIV-related fat redistribution. Leuprolide treats prostate cancer and endometriosis. Cyclosporine, used to prevent organ rejection after transplants, is a cyclic peptide.
In 2023, roughly 16% of new FDA drug approvals were peptide-based. That's not a niche.
These compounds share a molecular category with gray-market research peptides sold online. That's where the similarity ends. They've been through clinical trials. Dosing is standardized. Manufacturing is regulated. Purity testing is enforced. None of that applies to what comes next.
Research peptides
The third category is the most complicated, and the one driving most of the current noise.
Research peptides have biological plausibility and often promising animal data, but haven't completed the clinical trial process required for FDA approval. BPC-157, TB-500, Ipamorelin, CJC-1295, Epitalon, Semax, and Melanotan II all live here. Most of what circulates in fitness and longevity communities falls in this group.
The evidence is genuinely uneven.
A 2025 systematic review of BPC-157 found 36 relevant studies: 35 were animal studies and 1 was a human trial. Animal data doesn't reliably predict human outcomes. The confidence circulating online about BPC-157 in humans isn't connected to clinical evidence in any meaningful way.
Many compounds that worked well in rodents have failed in people. Some of these peptides were previously accessible through compounding pharmacies with a doctor's prescription. The FDA ended that in 2023, moving 19 peptides into a category designating significant safety concerns. As of April 2026, 12 of those 19 have been removed from the restricted list. FDA advisory committee meetings in July 2026 will evaluate whether compounding access should be restored. Right now these compounds sit in regulatory limbo: not fully banned, not yet approved for compounding.
For the current state of legal access, the legal status of research peptides has the breakdown.
What peptides are not
Peptides are not anabolic steroids. Steroids are structurally unrelated: derived from cholesterol, not amino acids. They enter cells and modify gene expression directly, and many suppress the body's natural hormone production in the process. Peptides bind to cell-surface receptors and send signals. They don't modify gene expression the same way, and most don't suppress testosterone production the way exogenous steroids do. The association comes from gym culture, not from chemistry. The full comparison between peptides and steroids covers this in detail.
Peptides are not human growth hormone. Growth hormone-releasing peptides like Ipamorelin, GHRP-2, and CJC-1295 stimulate the pituitary to produce more of its own GH. They are not GH. Administering actual human growth hormone is a different intervention with a different risk and regulatory profile.
Peptides are not safe because they're "natural." This is probably the most consequential wrong idea in this space. Insulin, oxytocin, and GLP-1 are natural. A molecule's origin tells you very little about its safety at therapeutic doses, especially when sourced from unregulated vendors. A certificate of analysis showing 99% purity means the compound is chemically what it claims to be. It says nothing about sterility, dosing accuracy, or bacterial contamination. Those are separate questions, and they don't answer themselves.
Why everyone is suddenly talking about peptides
Three things happened in a short period.
GLP-1 drugs put "peptide" into everyday vocabulary. When Ozempic became a cultural moment, millions of people learned that a peptide drug could produce dramatic effects on body weight. That created an audience willing to believe other peptides might do comparable things, including muscle recovery, aging, or injury healing. The reasoning doesn't follow scientifically. An extraordinary result from one compound, developed over decades and tested in large clinical trials, tells you almost nothing about a structurally unrelated compound with a few rat studies behind it. But the cultural spillover happened, and it's real.
A regulatory shift is underway. In 2023, the FDA restricted 19 peptides from compounding, cutting off physician-supervised access to compounds like BPC-157 and TB-500. In early 2026, HHS Secretary RFK Jr. publicly pushed to reverse those restrictions, and the FDA scheduled advisory committee meetings for July 2026 to evaluate restoring compounding access. Whatever the committee recommends will determine whether physicians can legally prescribe these compounds again through licensed pharmacies.
And social media. The gap between "animal studies look promising" and "this will heal your tendons" has never been smaller. Compounds with essentially no human trial data get discussed with the confidence of established drugs. That gap is what this site is built around.
Frequently asked questions
It depends on which peptide, at what dose, delivered how, and sourced from where. FDA-approved peptide drugs (insulin, GLP-1s, tesamorelin) have established safety records built through clinical trials. Topical skincare peptides carry minimal risk. Research peptides from gray-market vendors carry genuine unknowns: contamination risks, dosing inconsistencies, and long-term effects that no one has systematically studied in humans.
The "natural" framing doesn't help here. Peptides break down into amino acids, which sounds reassuring, but a peptide can still cause harm at a given dose before it breaks down. A full look at the evidence by category is in are peptides safe?
Depends on which peptide for which purpose. GLP-1 drugs have exceptionally strong clinical trial data. Collagen peptides have solid evidence for skin elasticity and joint outcomes. Specific skincare peptides like Matrixyl and GHK-Cu have clinical trial support for modest but measurable improvements.
Research peptides for performance, healing, or longevity? Almost entirely animal data. That doesn't mean they don't work; it means rigorous human evidence doesn't yet exist. Anyone claiming certainty about BPC-157 outcomes in people is running ahead of the actual research.
It varies, and the picture is actively changing. FDA-approved peptides are legal with a prescription. Topical peptides are legal as cosmetics. Most gray-market research peptides occupy a legal gray zone: technically permissible to purchase as research chemicals, but not legal to use for human health purposes. The FDA's April 2026 regulatory changes and the upcoming July 2026 advisory committee meetings may expand physician-supervised access. Full details are in the current legal status of research peptides.
No. Anabolic steroids are derived from cholesterol and work by entering cells and modifying gene expression, which often suppresses natural testosterone production. Peptides bind to cell-surface receptors and send signals. They're structurally unrelated and work through different mechanisms. The confusion comes from fitness culture, not the science. A full comparison between peptides and steroids is here.
For most research and therapeutic peptides, yes, because oral peptides break down in the gut before reaching their target. Collagen peptides are the notable exception, but they work through amino acid supply rather than receptor signaling, which is a different mechanism. Some peptides can be delivered nasally or sublingually, and delivery science is improving. If you're exploring a specific peptide for a specific goal and hoping to avoid injections, that needs to be a real conversation with a physician, not an assumption that an oral version exists.
Published by the PEPVi editorial team. Read our editorial standards.