
Three very different things all called "peptides"
Before you can assess safety, you need to know which category you're dealing with.
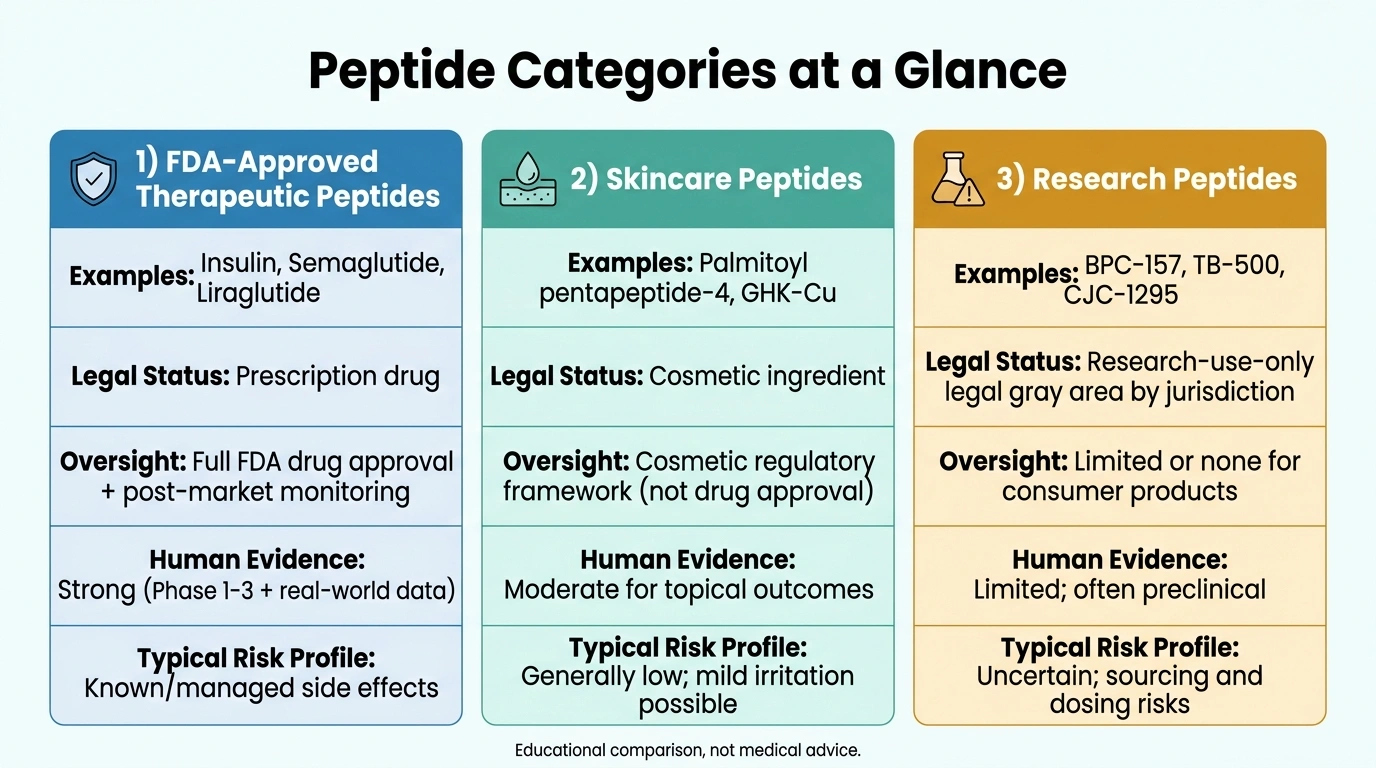
FDA-approved therapeutic peptides are drugs. Insulin is a peptide. So are semaglutide (Ozempic, Wegovy), liraglutide, and a growing list of others. Over 80 peptide-based drugs are currently FDA-approved, accounting for roughly 11% of all new drug approvals since 2016. These went through Phase 1, 2, and 3 clinical trials. Their side effects are documented, their doses calibrated, their risks understood.
Skincare peptides sit at the other end of the risk spectrum. When palmitoyl pentapeptide-4 shows up in a $40 serum, it's applied to the surface of your skin. It doesn't enter your bloodstream. Multiple clinical studies on topical peptides have found no serious adverse reactions. The worst you're likely to see is mild redness in sensitive or acne-prone skin, and that's rare. These peptides work (or don't work) locally, and the safety record is clean.
Research peptides are the gray zone. These are the ones showing up on peptide forums and in wellness communities: BPC-157, CJC-1295, ipamorelin, TB-500, selank, and dozens of others. Sold online, often shipped from overseas, used by people injecting themselves at home. The science behind some of them is genuinely interesting. The safety picture is genuinely incomplete.
If you're still fuzzy on what peptides are and how they work, that's worth reading first. The mechanism behind peptides explains why source and dose matter as much as they do.
What "research peptide" actually means
The term sounds like a cutting-edge compound in active development. What it actually means, legally, is "for laboratory use only, not for human consumption."
Research peptides carry an RUO designation: Research Use Only. Manufacturers sell them as laboratory reagents, chemical tools for studying cellular pathways in test tubes and animal models. That's the legal framing. The actual buyer is often a person who wants to heal a tendon or test a longevity protocol.
This matters for safety because RUO status means no regulatory oversight of what goes into the vial. There's no FDA inspection, no manufacturing standards, no requirement to disclose what's actually in the product. An independent analysis of unregulated peptides found roughly 25% were mislabeled, meaning a vial labeled as one peptide actually contained a different compound entirely. Contamination with heavy metals, incorrect concentrations, and undisclosed additives are all documented problems.
This isn't hypothetical. One documented case involved acute pancreatic failure after someone took high doses of an unapproved GLP-1 for weight loss. Cases of kidney failure have been linked to melanotan II. These aren't common, but they're real, and they happened to people who thought they were being careful.
The phrase "not for human consumption" on the label doesn't protect you legally or medically. It's a seller's liability shield.
Side effects by delivery method
Side effects vary significantly by how a peptide is taken. The delivery route determines absorption, concentration, and what parts of the body the compound actually reaches.
Topical peptides
Topically applied peptides have the safest profile of any category. Clinical trials on skincare peptides have reported no serious adverse events across hundreds of participants. The most common complaint is mild redness in people with reactive skin. If your skincare routine includes retinoids or exfoliating acids, those are more likely to irritate than the peptides in the same product.
GHK-Cu, one of the more studied topical peptides, has been tested in randomized controlled trials without safety concerns. If you want the lowest-risk entry point into peptides, topical is it.
Oral peptide supplements
Collagen peptides, sold as powders and pills, are the most common oral form. They're generally well-tolerated. Some people experience mild GI effects (bloating, loose stools) when starting. The bigger concern with oral peptides isn't safety, it's absorption. Most peptide chains break down in the digestive tract before they can act systemically. Collagen peptides work partly because they serve as a direct amino acid source for skin tissue, not because an intact peptide chain is reaching your cells.
The safety concern with oral supplements isn't the peptides themselves. It's the supplement industry. The FDA doesn't require pre-market approval for supplements, so what's on the label isn't always what's in the bottle. Buy from brands that publish third-party testing, not just manufacturers who claim to.
Injectable peptides (FDA-approved)
The most common injectable peptides with solid safety data are the GLP-1 receptor agonists. Their side effect profile is well-established.
Nausea affects 14–28% of users, diarrhea hits 8–20%, and vomiting occurs in 6–12%. These effects are most pronounced during dose escalation and typically ease over time. Pancreatitis is rare, occurring at rates comparable to placebo in clinical trials.
Injection site reactions (redness, swelling, minor pain) are common across all injectable peptides and usually temporary. Rotating injection sites helps.
For FDA-approved injectables taken under physician supervision, the risk-benefit calculation is the same as any medication: documented side effects weighed against documented benefits. See what peptides can actually do for a goal-by-goal look at what the evidence shows.
Injectable research peptides
This is where the safety picture gets genuinely murky. The peptides themselves may or may not cause harm. For many of them, we simply don't know, because adequate human trials don't exist. What compounds the risk is the sourcing problem: contamination, mislabeling, and dosing errors.
Dosing errors with injectables can be serious. Insulin syringes measure volume, not mass. Confusing micrograms with milligrams means potentially injecting 1,000 times the intended amount. Reddit forums contain reports of intense anxiety, dissociation, unexpected hormonal effects, and prolonged side effects from research peptide use, most of which can't be traced to a specific mechanism because there are no human trials to reference.
Understanding how peptides signal cells helps put this in context. Compounds that influence growth hormone release, tissue repair, or immune function are biologically active. Their effects don't always stay limited to what you're targeting.
Red flags when buying peptides online
A few things are worth checking before you trust a vendor.
- Certificate of Analysis: A real COA is batch-specific — it's tied to the lot number you're actually buying. A document that matches every product on the site tells you nothing about what's in your vial.
- No prescription required: If a US vendor ships injectable peptides without requiring a physician's prescription, they're operating outside the law. That's not a minor technicality; it tells you something about how they handle everything else.
- "Not for human consumption" labeling: Products with this label are selling research-grade material, not pharmaceutical-grade. That language exists to protect the seller legally. It says nothing about product quality.
- Third-party testing: Internal manufacturer claims are not independent verification. Look for HPLC analysis from a named external lab, with labeled axes and the testing methodology stated.
- Price dramatically below market: Something about the product is different. Pharmaceutical-grade peptides cost real money to produce and test properly. There's no shortcut.
The July 2026 reclassification: what changes and what doesn't
Since late 2023, many popular research peptides, including BPC-157, TB-500, CJC-1295, ipamorelin, and others, have been on the FDA's Category 2 list, a designation that blocks licensed compounding pharmacies from preparing them.
In April 2026, the FDA formally removed 12 peptides from that list. The agency's advisory committee meets in July 2026 to review BPC-157, TB-500, thymosin alpha-1, and several others.
If those peptides land on the 503A bulk drug substances list after those meetings, licensed compounding pharmacies can legally prepare them under physician prescription. That's a real shift. These compounds would move from unregulated gray-market products to pharmacy-prepared formulations with manufacturing standards, lot testing, and medical oversight.
What doesn't change is the underlying science. None of these peptides will be FDA-approved. They still won't have completed Phase 3 human trials. Compounding is a pathway for physicians to prescribe off-label compounds through regulated facilities, not an approval process. The reclassification improves the safety infrastructure. The science is still missing, and the reclassification doesn't change that.
When to talk to a doctor
Talk to a doctor before you start injectables, not after you've already ordered. A physician can check your current medications for interactions, flag conditions that make peptide use risky, and, if they know their way around peptides, help you source from a regulated pharmacy rather than a gray-market vendor.
If something unexpected happens after starting, get it evaluated: unusual swelling, heart palpitations, severe injection site reactions, or effects that feel out of proportion to your dose. It probably isn't serious, but these things warrant a look.
Two situations call for extra care. If you have a personal or family history of cancer, some peptides influence growth signaling pathways, and the theoretical concern about accelerating undiagnosed cell growth isn't settled enough to ignore. And if you're taking other medications, "derived from amino acids" doesn't mean non-interacting. Peptides can conflict with hormonal therapies, blood pressure medications, and diabetes drugs in ways that aren't obvious.
What makes a source trustworthy
Licensed compounding pharmacies, 503A or 503B, are the right starting point. They operate under state pharmacy board oversight, prepare peptides with verified purity and potency, and require a physician prescription. Once the July 2026 reclassifications take effect, several popular peptides should be accessible through this pathway.
For compounds not yet available through a compounding pharmacy, a vendor with batch-specific COAs from a named independent laboratory is the closest approximation of accountability available. It's not pharmacy-grade, but it's meaningfully better than nothing.
Physician-supervised clinics that source from regulated pharmacies offer the full picture: medical screening, verified compounds, and someone to call if something goes wrong. The quality gap between peptide clinics is real, and it's not always visible from their websites. Choosing a provider thoughtfully is worth your time.
Frequently asked questions
For FDA-approved peptides like GLP-1 agonists, the long-term profile is reasonably understood: clinical trials and real-world use now span several years. For research peptides, long-term human data is essentially absent. Six months without obvious problems is not long-term safety data. It's a single data point.
It depends on the type. Injectable GLP-1 peptides cause GI effects in a lot of users. Nausea is most frequent, affecting 14–28% of people, and typically improves after the dose-escalation phase. Topical peptides rarely cause anything beyond mild redness. Research injectables have a poorly documented side effect profile; injection site reactions and the sourcing concerns above are the main documented risks.
No. Peptide therapy typically means medically supervised injectable treatments targeting specific goals: injury recovery, hormone support, immune function. Peptide supplements are over-the-counter products, usually oral, with lower bioavailability and different mechanisms. The safety profiles, costs, and oversight involved are different in almost every way.
No universal answer here. Some peptides interact with hormonal therapies, diabetes medications, or blood pressure drugs. If you're on any prescription medication, talk to a physician before starting. That's exactly the conversation this situation calls for.
It moves certain peptides from an unregulated gray market toward a supervised, pharmacy-based system with manufacturing standards, verified purity, and physician oversight. All of that reduces risk. What it doesn't do is generate human clinical trial data. The reclassification improves access and infrastructure; the evidence gaps remain.
Published by the PEPVi editorial team. Read our editorial standards.