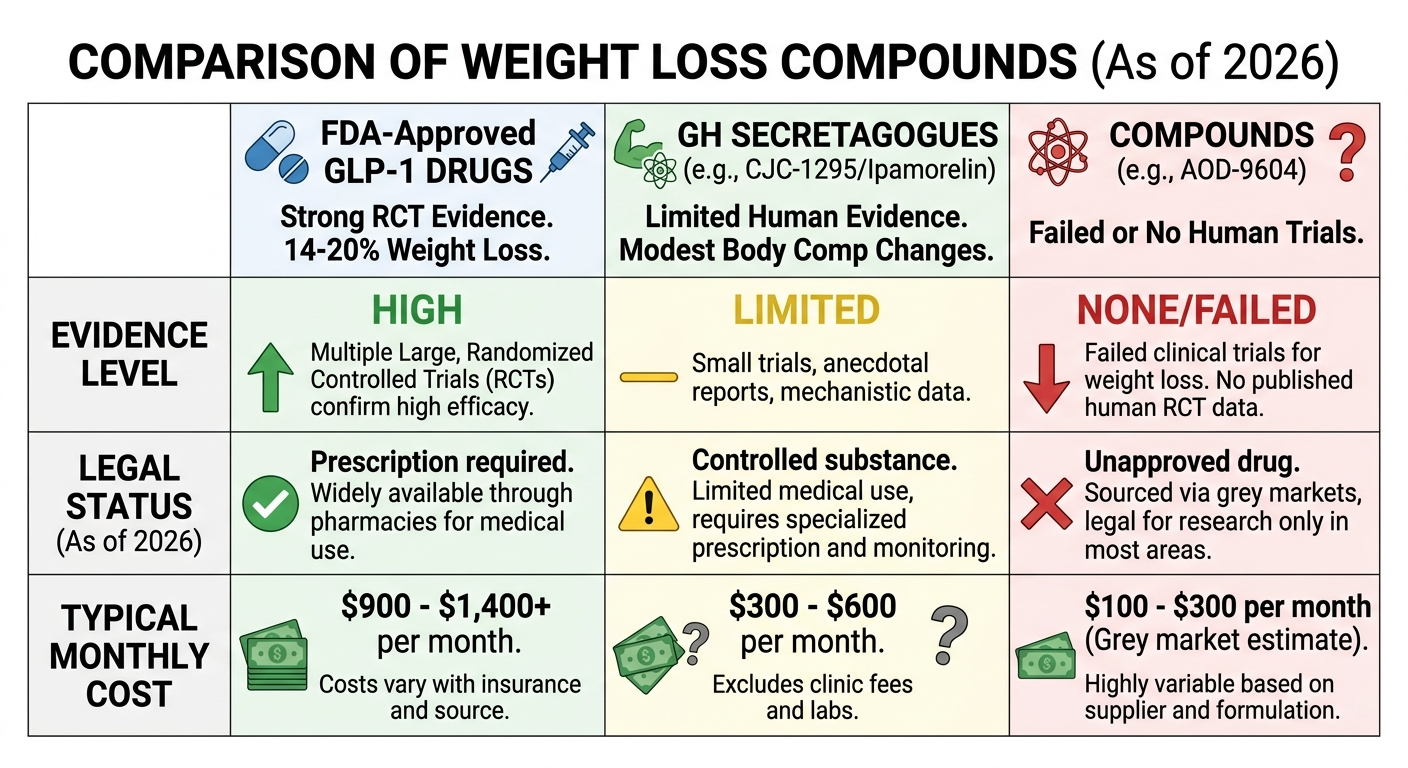
Some peptides produce real weight loss. The GLP-1 trial data is good: 14 to 20 percent average body weight reduction, across tens of thousands of patients. Other things sold in the "peptides for weight loss" bucket have mostly animal studies behind them, and some have already failed in human trials.
"Peptide" is a molecular category, not a drug class — a distinction worth clearing up before anything else.
How peptides affect metabolism and appetite
Your body uses peptides to manage hunger and fat storage right now, without any supplements involved. GLP-1, ghrelin, leptin. These are all peptides, and they're doing the basic work of signaling when you've eaten, how much fat to store, and when to stop.
When you eat, your gut releases GLP-1. It tells your pancreas to release insulin, tells your brain you're full, and slows how fast food moves through your stomach. Researchers have spent decades trying to extend or mimic that combination because when it works, it produces sustained reductions in calorie intake without relying on willpower.
Growth hormone secretagogues take a different route. CJC-1295 and Ipamorelin stimulate the pituitary to release more growth hormone, which in turn promotes fat breakdown and helps maintain lean muscle. The effect on total body weight is modest. The mechanism is real, but it's not a GLP-1 analog. These are different tools solving different problems.
What peptides are and how they signal cells goes into the biology in more depth.
GLP-1 peptides explained simply
Natural GLP-1 breaks down in about two minutes. That's the problem the drugs solve. Semaglutide, liraglutide, and tirzepatide are all engineered to bind the same receptor but resist degradation, staying active for days or a week at a time.
In practice, the effect people notice most is what some call "food noise" going quiet. GLP-1 receptors in the hypothalamus get activated, and the constant background thinking about food (what to eat, when to eat, wanting to eat again 90 minutes after a meal) fades out for many users. This isn't appetite suppression in the willpower sense. For people who've lived with it, the food noise stopping feels genuinely strange.
The drugs also slow gastric emptying and help regulate post-meal blood sugar. Those contribute to the weight loss, but the food noise reduction is probably the biggest piece.
Tirzepatide (Zepbound) adds GIP receptor activation on top of GLP-1. GIP is involved in fat storage and energy metabolism. That second mechanism is why tirzepatide consistently outperforms semaglutide. In SURMOUNT-5, tirzepatide hit 20.2% average weight loss versus 13.7% for semaglutide at 72 weeks.
For a direct comparison of the approved options, semaglutide vs. tirzepatide for weight loss covers the tradeoffs.
Pharmaceutical GLP-1s vs. research peptides: not the same thing
Wegovy, Ozempic, and Zepbound ran through large clinical trials before they reached patients. The semaglutide STEP program enrolled over 17,000 people: standardized dosing, independent safety oversight, peer-reviewed data. Years of process and billions of dollars produced what we know about those drugs.
Research peptides haven't done that. Most have no completed human trials. Dosing isn't standardized anywhere. What you actually get depends entirely on who made it and where it was stored.
AOD-9604 is worth knowing as a cautionary example. It's a fragment of human growth hormone that looked genuinely promising in animal fat loss models, compelling enough to fund Phase 3 trials. Those trials, in humans, failed. There's no peer-reviewed evidence that it produces meaningful weight loss in people. Plenty of wellness sites still list it as a proven fat-loss compound. They're citing preclinical data or nothing.
CJC-1295 and Ipamorelin hold up better. They do reliably increase growth hormone and IGF-1 in humans, which shifts body composition over time: less visceral fat, somewhat more lean mass. But the research is mostly in growth-hormone-deficient patients, not healthy people with excess weight, and the synergistic stacking effects people expect from combining them haven't been directly studied. The honest expectation is gradual improvement in body composition, not dramatic weight loss.
Types of peptides has a broader look at where different categories sit on the evidence spectrum.
Realistic expectations
Semaglutide 2.4 mg weekly averaged 14.9% body weight reduction over 68 weeks in the STEP 1 trial, with lifestyle support included. Tirzepatide 15 mg averaged 20.2% at 72 weeks in SURMOUNT-5. Those are population averages; individual results vary, and about 20 to 30% of users don't respond well.
Two things consistently get undersold: rebound weight after stopping, and muscle loss during treatment.
SURMOUNT-4 data showed patients who stopped tirzepatide regained roughly two-thirds of lost weight within 12 months. Semaglutide shows similar rebound. These drugs work while you're on them. The picture after stopping is not so clean.
Muscle loss is the other issue. When calorie intake drops fast, the body breaks down both fat and lean tissue. Studies estimate that around 25 to 40% of the weight lost on GLP-1 drugs is lean mass rather than fat. For people who want long-term metabolic health, not just a lower number on the scale, this matters. Resistance training during a GLP-1 protocol reduces lean mass loss significantly — skipping it means giving up a meaningful part of what makes the results durable.
CJC-1295 and Ipamorelin? More modest: body composition shifts over months, better sleep quality, faster recovery, some reduction in visceral fat. The people promising dramatic weight loss from GH secretagogues without GLP-1s are ahead of what the data shows.
Research peptides for fat loss goes deeper on the non-GLP-1 options.
Safety
The GLP-1 side effect profile is well-documented at this point. Nausea affects roughly 37 to 44% of users, worst during dose escalation and usually improving after a few weeks. Vomiting, constipation, diarrhea, and fatigue are also common. Discontinuation rates in clinical trials were notable; this doesn't work for everyone.
Beyond GI effects: these drugs carry a black-box warning for anyone with a personal or family history of medullary thyroid carcinoma or MEN2, based on findings in rodent studies. Pancreatitis is rare but documented. Gallbladder problems have been reported.
Something that doesn't get enough coverage: GLP-1 drugs can disrupt menstrual cycles. Irregular periods, intermenstrual bleeding, and heavier cycles showed up in a 2026 study that analyzed over 400,000 self-reported Reddit posts on GLP-1 side effects. This wasn't a minor finding buried in footnotes — it appeared consistently. Women starting these drugs should know this going in, not discover it three months later.
For research peptides, the safety situation is different in kind: not well-understood danger, just genuine unknowns. Short-term and injection-site profiles of CJC-1295/Ipamorelin look acceptable in available literature. Long-term effects in humans haven't been established because the studies haven't been done.
If you have active cancer, thyroid conditions, or a history of pancreatitis, GLP-1 use needs a real physician conversation. Are peptides safe covers risk by category. What peptide therapy looks like in clinical practice — what labs get run, what oversight actually means — is also useful context.
What changes in July 2026
In April 2026, the FDA moved 12 to 14 peptides off its restricted compounding list, including CJC-1295, Ipamorelin, and BPC-157. They're back in Category 1, which means licensed compounding pharmacies can prepare them again under a physician's prescription. The FDA's Pharmacy Compounding Advisory Committee meets July 23–24, 2026 to formally review these compounds.
For weight loss purposes, this restores something that was cut off in 2023: the ability to get GH secretagogues through a legitimate physician-supervised channel rather than the gray market.
What it doesn't do: these are still not FDA-approved drugs. No clinical trials were completed. Reclassification opens compounding access under proper medical oversight, not over-the-counter purchase. Anyone representing it that way is cutting corners on the explanation.
The semaglutide compounding story is separate and already closed. The shortage that allowed cheaper compounded copies ended when the FDA declared it resolved in February 2025. Compounded semaglutide is not legally available outside very narrow circumstances.
What RFK's peptide reclassification actually means has the full details.
Medically supervised options worth considering
If you've decided a peptide-based weight loss program makes sense for you, the three providers below are worth a look. Prioritize physician oversight, pharmacy transparency, and clear pricing before you commit.
TrimRx
TrimRx focuses on GLP-1 weight loss care rather than broad hormone programs. You get physician review, medication through an FDA-registered pharmacy, and ongoing dose support in one program.
Best for: People who want a focused GLP-1 platform with straightforward onboarding and clear pricing.
Pros
- Purpose-built for GLP-1 weight loss
- Physician-reviewed intake before prescribing
- FDA-registered pharmacy sourcing
- Dose support and follow-up included
Good to know
- Newer platform than some legacy telehealth brands
- GLP-1 focused, so limited fit if you want GH secretagogues
PEPVi may earn a commission at no cost to you.
PeterMD
PeterMD offers lower-cost GLP-1 access and also supports GH secretagogue programs. Intake runs through Quest labs with licensed provider review and medication shipped to your door.
Best for: Value-focused patients who are comfortable with an asynchronous workflow and may want both GLP-1s and GH secretagogues.
Pros
- Among the lowest GLP-1 entry prices in this category
- Access to both GLP-1s and GH secretagogues
- Fast Quest-based intake with licensed review
- Accepts HSA and FSA cards
Good to know
- Asynchronous care model rather than live physician calls
- Not available in California, Texas, and several other states
State availability: Check their site for the latest non-serviceable states before you start.
PEPVi may earn a commission at no cost to you.
Oak Longevity
Oak Longevity offers GLP-1s alongside compounding peptides like CJC-1295 and Ipamorelin under one physician-supervised platform. Their compounding pharmacy is fully independent with no ownership stake, and every batch is tested for purity, potency, and sterility before shipping. Intake runs async through a short health form, with physician review typically within hours and medication shipped within a few days.
Best for: Patients who want GLP-1 access and the option to stack GH secretagogues under the same provider.
Pros
- Independent 503A pharmacy with no ownership stake; every batch tested for purity, potency, and sterility
- GLP-1s and GH secretagogues (CJC-1295, Ipamorelin) available in one program
- Program fee and medication cost billed separately, with medications at cost
- Async intake, no required video call, physician review typically within hours
Good to know
- No anti-nausea medications included in the protocol
- Peptide protocol pricing not publicly listed; requires direct inquiry
- Newer platform with limited third-party review history
PEPVi may earn a commission at no cost to you.
Frequently Asked Questions
GLP-1 drugs, specifically semaglutide (Wegovy) and tirzepatide (Zepbound), have solid trial data: 14 to 20% average body weight reduction over 68 to 72 weeks. Research peptides like CJC-1295 and Ipamorelin produce real changes in body composition through GH stimulation, but the effect is modest: better fat distribution and lean mass, not dramatic total weight loss. "Peptides for weight loss" covers both categories. They're not otherwise comparable.
Ozempic went through Phase 3 clinical trials before approval: over 17,000 patients in the STEP program alone, standardized dosing, regulated manufacturing, documented safety. CJC-1295 and Ipamorelin didn't go through that. As of April 2026 they're available via compounding pharmacy with a prescription, but a prescription doesn't substitute for trial data. Different mechanisms, different evidence base, not interchangeable.
For GLP-1 drugs, probably. SURMOUNT-4 found tirzepatide patients regained roughly two-thirds of lost weight within 12 months of stopping. Semaglutide shows similar rebound patterns. The drugs seem to work while you're taking them. That reality should factor into anyone's decision before they start. For research peptides, there's essentially no controlled data to cite. There just aren't enough human trials.
Yes. GLP-1 drugs make eating less significantly easier: the food preoccupation drops, portions naturally get smaller. But nutrition quality still matters, especially because the muscle loss from fast caloric restriction is real. Every major semaglutide and tirzepatide trial included structured lifestyle support alongside medication. Real-world outcomes without it tend to be lower. Resistance training specifically buffers the lean mass loss that happens on GLP-1 protocols.
Research-grade peptides get sold online as "research chemicals" through a legal gray area, no prescription needed. Using them for weight loss that way means no quality control, no medical oversight, and no standardized dosing. FDA testing has found contamination and dosing errors in a notable share of tested compounded peptide products. FDA-approved GLP-1 drugs require a prescription. Compounded CJC-1295 and Ipamorelin require a physician's prescription through a licensed pharmacy as of April 2026. The gray market exists. It's not the same as medical supervision.
Sources
- Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1) — NEJM 2021; documents 14.9% average body weight reduction over 68 weeks that is the benchmark for semaglutide efficacy in weight loss
- Tirzepatide vs. Semaglutide in Obesity (SURMOUNT-5) — NEJM; head-to-head trial showing tirzepatide's 20.2% vs. semaglutide's 13.7% weight loss at 72 weeks
- The Role of GLP-1 in Energy Homeostasis and Treatment of Obesity — PMC; explains the central and peripheral mechanisms by which GLP-1 suppresses appetite and reduces caloric intake
- GLP-1 Receptor Agonists: A Review of Head-to-Head Clinical Studies — PMC; comparative review of GLP-1 RA mechanisms and relative efficacy across trials
- Prolonged Stimulation of Growth Hormone and IGF-1 Secretion by CJC-1295 — PubMed 2006; documents CJC-1295's effects on GH and IGF-1 levels, foundational evidence for its body composition use
- Ipamorelin, the First Selective Growth Hormone Secretagogue — PubMed 1998; original pharmacological characterization of ipamorelin's selective GH secretagogue activity and favorable safety profile
- Effects of Growth Hormone Secretagogues on Body Composition and Metabolism — PMC; reviews evidence for GH secretagogues in reducing visceral fat and improving lean body mass
- Safety and Tolerability of Semaglutide Across SUSTAIN and STEP Programs — PubMed; pooled safety analysis covering GI adverse events, pancreatitis, and thyroid findings across thousands of trial participants
- Self-Reported Side Effects of Semaglutide and Tirzepatide in Online Communities — Nature Health 2026; AI analysis of 400,000+ Reddit posts documenting real-world side effects including underreported menstrual disruption
- FDA Announces Removal of 12 Peptides from Category 2 (Orrick, April 2026) — regulatory analysis explaining the April 2026 reclassification and July 2026 PCAC meeting schedule
- Research and Prospect of Peptides for Use in Obesity Treatment — PMC; academic review of endogenous peptides (GLP-1, leptin, ghrelin) and their roles in obesity pathophysiology
- Weight Regained Within 18 Months of Stopping GLP-1 Drugs (SURMOUNT-4 data) — documents the two-thirds weight regain within 12 months of stopping tirzepatide
Published by the PEPVi editorial team. Read our editorial standards.