
Peptide therapy for weight loss, the clinical kind, means a GLP-1 medication from a licensed physician with bloodwork first and monitoring built into the program. The evidence behind it is good: the STEP 1 trial showed 14.9% average weight loss over 68 weeks with semaglutide, and tirzepatide has since pushed past 20%.
Whether it's right for you depends on your BMI, your health history, and what you're willing to spend.
Which peptides are used clinically for weight loss
Most of the time, when a physician prescribes peptide therapy for weight loss, they mean one of two GLP-1 receptor agonists: semaglutide or tirzepatide.
Semaglutide (brand names Wegovy for weight loss, Ozempic for diabetes) mimics GLP-1, a gut hormone your body releases after eating. It tells your brain you're full, slows gastric emptying, and dials down the constant background food preoccupation many patients call "food noise." At the 2.4 mg weekly dose, the STEP 1 trial found that nearly 87% of patients lost at least 5% of their body weight over 68 weeks, and 50% lost 15% or more.
Tirzepatide (Zepbound for weight loss, Mounjaro for diabetes) activates both GLP-1 and GIP receptors. GIP is a second incretin hormone involved in fat storage and energy metabolism. That second mechanism is why tirzepatide consistently outperforms semaglutide: in SURMOUNT-1, the 15 mg dose produced 20.9% average weight loss over 72 weeks, and 57% of patients lost at least 20% of their body weight.
Growth hormone secretagogues (CJC-1295, Ipamorelin, Sermorelin) come up in some clinical weight programs, but they work differently and produce different results. They stimulate the pituitary to release more growth hormone, which shifts body composition over time: less visceral fat, somewhat more lean mass. The effect on scale weight is modest. Some physicians stack them alongside GLP-1s in broader metabolic protocols, but if the goal is meaningful weight loss by number, GLP-1s are doing the work.
If you're new to what peptides are and how they work in the body, the beginner's guide to peptides covers the basics first. The guide to peptide types covers where different categories sit on the evidence spectrum. For a direct comparison of semaglutide and tirzepatide, the head-to-head breakdown covers the trial data and practical tradeoffs.
What a clinical program actually looks like
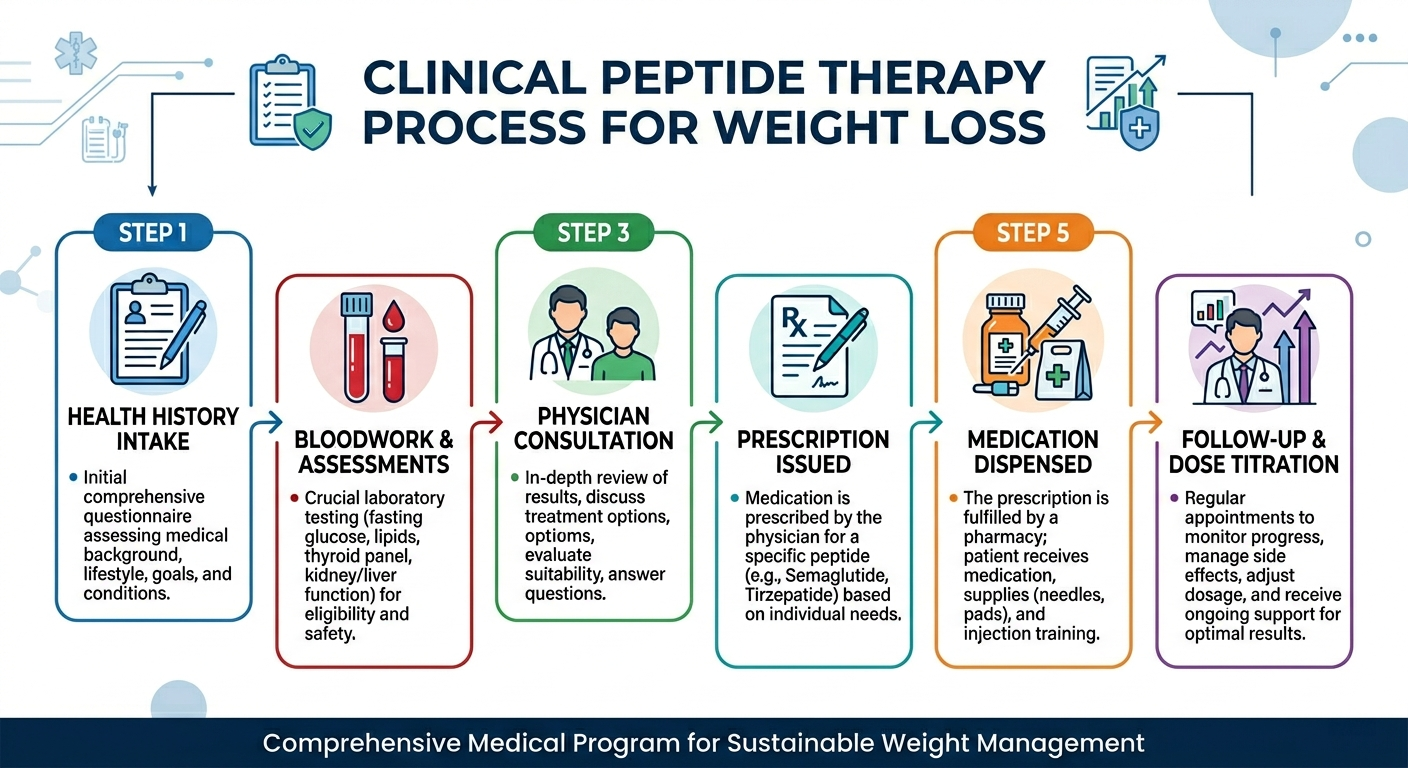
A well-run program follows a consistent sequence whether you go through a local physician or a telehealth platform.
Intake and health history. You fill out a detailed medical history covering diagnoses, medications, family history (especially thyroid cancer and pancreatitis), and what you're trying to achieve. GLP-1 medications carry a black-box warning for anyone with a personal or family history of medullary thyroid carcinoma or MEN2 syndrome. A physician who skips this step is cutting a corner that could matter.
Bloodwork. Before prescribing anything, a responsible provider orders labs: typically a metabolic panel, thyroid function, lipid panel, and fasting glucose or HbA1c. These establish your baseline and screen for contraindications. Lab costs run $100–$350 out of pocket at most platforms, though some include them in the first-month fee.
Initial consultation. 20 to 45 minutes, video or in-person. The physician reviews your labs and history, proposes a starting dose, and walks through the titration plan. Most programs start semaglutide at 0.25 mg weekly and increase every four weeks. Tirzepatide starts at 2.5 mg and follows a similar stair-step. Going too fast is the most common reason people stop early from GI side effects, so slow titration matters.
Medication dispensed. The prescription goes to a compounding pharmacy (for compounded versions) or a retail pharmacy (for branded). Branded Wegovy and Zepbound come as auto-injectors. Compounded versions arrive as a multi-dose vial with syringes.
Follow-up and dose adjustments. This is where programs diverge most. A good one includes check-ins at 4–6 weeks to assess how you're tolerating the dose and adjust if needed. Labs get repeated at 3 months and again at 6 months. Providers who go dark after the first shipment are collecting subscription fees without running a clinical program.
For more on what labs get run and how to evaluate a provider, see the full breakdown of what peptide therapy involves.
Who qualifies
The FDA-approved eligibility criteria for semaglutide (Wegovy) and tirzepatide (Zepbound) are the same: a BMI of 30 or higher, or a BMI of 27 or higher with at least one weight-related comorbidity such as type 2 diabetes, hypertension, high cholesterol, obstructive sleep apnea, or cardiovascular disease.
Those thresholds come directly from the clinical trial enrollment criteria. The SURMOUNT-1 trial enrolled 2,539 adults meeting exactly these criteria, excluding people with type 2 diabetes. That's where the evidence exists.
Some telehealth platforms apply lower BMI thresholds or broader comorbidity definitions. That's a business decision, not a clinical standard. If a platform prescribes without reviewing labs and health history, that's worth noting regardless of your BMI.
A few other factors affect whether a physician will prescribe:
Thyroid history. GLP-1 medications are contraindicated in people with a personal or family history of medullary thyroid carcinoma or MEN2. This applies to every drug in this class.
Pancreatitis history. Active pancreatitis rules out GLP-1s. Prior history warrants careful evaluation.
Active cancer. Peptides that stimulate tissue growth are contraindicated with active cancer or certain cancer histories. A real consultation covers this.
Current medications. GLP-1s can interact with insulin and certain diabetes drugs in ways that require dose adjustment. Your full medication list needs to be part of intake.
The safety guide covers contraindications in more detail across different peptide types.
What it costs
Most articles on peptide therapy skip the cost question. It shouldn't be skipped.
Branded medications at retail without insurance: Wegovy (semaglutide 2.4 mg) runs approximately $1,349/month. Zepbound (tirzepatide) runs $1,059–$1,159/month depending on dose. Both manufacturers have direct-to-patient programs: NovoCare for Wegovy and LillyDirect for Zepbound can bring costs to $299–$349/month for patients without insurance or who can't get prior authorization approved.
Compounded medications via telehealth: Compounded semaglutide runs $99–$299/month. Compounded tirzepatide runs $349–$499/month. The compounded semaglutide price is narrowing. The FDA declared the semaglutide shortage resolved in February 2025 and has been restricting large-scale compounding of it since. Platforms still advertising rock-bottom prices may be operating in tighter regulatory territory than they let on.
Program costs on top of medication: Initial consultation: $0–$150 depending on the platform. Lab work: $100–$350. Monthly platform or membership fees: $25–$149/month at many telehealth clinics. Follow-up consultations: $50–$150 each if not included. A realistic 12-month cost for a properly supervised program runs $1,500–$5,000 depending on route and medication.
Insurance: Wegovy and Zepbound are covered by some commercial plans when you meet eligibility criteria, but coverage isn't guaranteed. Prior authorization requirements for weight-loss GLP-1s jumped from under 15% of large employer plans in 2023 to over 80% by 2024. Medicare started covering GLP-1s for weight loss in 2026 for high-risk patients.
The full cost breakdown covers what different platforms actually charge and where hidden fees tend to show up.
Telehealth options
Telehealth has made physician-supervised weight loss programs accessible without a local specialist. Quality varies, but the legitimate platforms run the same way a good in-person clinic does: labs first, real physician review, dose titration, ongoing follow-up.
Two things worth verifying before signing up anywhere:
Is there a licensed physician reviewing your case? Questionnaire-only intake with automated approval is not medical supervision. If you can get a prescription in five minutes without any clinical review, that's what you're buying.
Which compounding pharmacy do they use? A real platform names it and can confirm it holds 503A or 503B FDA registration. The FDA has found incorrect dosages or undeclared ingredients in up to 40% of tested online compounded peptide products. Sourcing matters.
Our guide to choosing a peptide provider has a broader evaluation of the major platforms.
TrimRx
TrimRx is built around physician-supervised GLP-1 care. Intake includes medical review, medication fulfillment through an FDA-registered pharmacy, and structured dose support after you start.
Best for: Patients who want a focused GLP-1 platform with transparent pricing before enrollment.
Pros
- GLP-1-focused care model with physician oversight
- FDA-registered pharmacy sourcing
- Follow-up and dose support included
- Pricing disclosed before commitment
Good to know
- Newer platform than legacy telehealth providers
- Less ideal if you want non-GLP-1 peptide options
PEPVi may earn a commission at no cost to you.
PeterMD
PeterMD combines lower-cost GLP-1 access with optional GH secretagogue programs. The workflow is lean: Quest lab intake, asynchronous licensed provider review, then direct-to-door medication shipping.
Best for: Value-focused patients comfortable with async care who may want both GLP-1 and GH-based options over time.
Pros
- Competitive GLP-1 pricing in this category
- Offers both GLP-1 and GH secretagogue programs
- Fast Quest-based intake process
- Accepts HSA and FSA cards
Good to know
- Asynchronous care rather than a live physician call flow
- Not available in California, Texas, and several other states
PEPVi may earn a commission at no cost to you.
Oak Longevity
Oak Longevity covers GLP-1s (semaglutide, tirzepatide) alongside compounding peptides like CJC-1295 and Ipamorelin under one physician-supervised platform. Their compounding pharmacy is fully independent with no ownership stake, and every batch is tested for purity, potency, and sterility before shipping. Intake is async: a short online health form, licensed physician review typically within hours, medication shipped within a few days.
Best for: Patients who want GLP-1 access and the option to add physician-supervised GH secretagogues under the same provider.
Pros
- Independent 503A pharmacy with no ownership stake; every batch tested for purity, potency, and sterility
- GLP-1s and GH secretagogues (CJC-1295, Ipamorelin) available in one program
- Program fee and medication cost billed separately, with medications at cost
- Async intake, no required video call, physician review typically within hours
Good to know
- No anti-nausea medications included in the protocol
- Peptide protocol pricing not publicly listed; requires direct inquiry
- Newer platform with limited third-party review history
PEPVi may earn a commission at no cost to you.
What changes in July 2026
In April 2026, the FDA removed 12 peptides from its Category 2 restricted list, restoring legal compounding access to compounds including CJC-1295, Ipamorelin, and BPC-157. The FDA's Pharmacy Compounding Advisory Committee meets July 23–24, 2026 to formally review these peptides, and their recommendations will shape compounding access going forward.
For weight loss specifically, the reclassification matters most for growth hormone secretagogue access. CJC-1295 and Ipamorelin are back in the legal compounding pathway under a physician's prescription, giving patients a legitimate channel for GH-based body composition protocols again.
GLP-1s are moving in a different direction. Compounded semaglutide access is tightening as the FDA enforces its ruling that the shortage is resolved. The cheap end of the compounded GLP-1 market is shrinking. The full breakdown of what the reclassification means has the regulatory details. For the broader picture of weight loss peptides and where the evidence is strong versus thin, the peptides for weight loss guide covers it.
Frequently Asked Questions
Functionally, they can be the same thing. Peptide therapy for weight loss through a licensed clinical program often means semaglutide (the active ingredient in Ozempic and Wegovy) or tirzepatide, prescribed under physician supervision. "Peptide therapy" is the clinical framing; Ozempic and Wegovy are brand names. The distinction that matters is the route (labs, real physician oversight, dose titration, follow-up) versus buying something online and dosing yourself.
The FDA-approved criteria require a BMI of 30 or higher, or 27 or higher with a comorbidity like hypertension, high cholesterol, or sleep apnea. Some telehealth platforms prescribe below those thresholds, but that puts them outside the evidence base the drugs were tested against. For someone with a BMI under 27 and no comorbidities, most responsible physicians won't prescribe a GLP-1 for weight loss. The trial data simply doesn't extend to lower-risk patients.
Most obesity medicine specialists treat these as long-term medications, not a finite course. The SURMOUNT-4 trial showed tirzepatide patients who stopped regained roughly two-thirds of their lost weight within 12 months. Semaglutide follows a similar pattern. The drugs manage weight while you take them. That's worth understanding before you start, not after.
The active molecule is the same, but manufacturing consistency is not guaranteed to be identical. The FDA's concern with compounded products is purity, inactive ingredients, and sterility. A platform sourcing from a reputable 503A or 503B pharmacy is operating through a legitimate clinical channel. One that can't name its pharmacy, or switches compounders without telling you, is a different situation. Ask before you subscribe.
Some commercial plans cover Wegovy or Zepbound for qualifying patients, but prior authorization is required at over 80% of large employer plans as of 2024, and denials are common. If prior auth is denied, manufacturer savings programs can bring branded drug costs to $299–$349/month for commercially-insured patients. NovoCare handles Wegovy; LillyDirect handles Zepbound.
Sources
- Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1) — NEJM 2021; primary efficacy data: 14.9% average weight loss, 86.4% of patients losing at least 5% body weight over 68 weeks with semaglutide 2.4 mg
- Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1) — NEJM 2022; 20.9% average weight loss at the 15 mg dose, 57% of patients losing at least 20% body weight; source for FDA eligibility criteria used throughout
- Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes (SELECT) — NEJM 2023; 17,604-patient trial showing 20% MACE reduction and clinical safety profile under physician supervision
- WHO Guideline on GLP-1 Therapies for Obesity in Adults — JAMA December 2025; first WHO guideline recommending GLP-1s as long-term treatment for obesity, with BMI and comorbidity eligibility framework
- Twelve-month real-world telehealth GLP-1 outcomes — Obesity 2024; 53,590 patients through a telehealth program achieving 19.4% average weight loss at 12 months; validates that telehealth delivery produces clinical-trial-comparable results
- GLP-1 RA efficacy and safety meta-analysis — Endocrine Practice 2024; pooled analysis of 15 randomized trials supporting cardiometabolic benefit claims and characterizing the GI side effect profile
- Net prices of new antiobesity medications — Obesity 2024; documents actual net monthly costs after manufacturer discounts and direct-to-patient program pricing
- Fiscal Impact of Expanded Medicare GLP-1 Coverage — JAMA Health Forum 2025; prior authorization surge from under 15% to over 80% of large employer plans; context for access and insurance discussion
- FDA Peptide Reclassification 2026 — Orrick regulatory analysis, April 2026; explains removal of 12 peptides from Category 2 and the July 2026 PCAC meeting schedule
- Self-Reported Side Effects of Semaglutide and Tirzepatide in Online Communities — Nature Health 2026; AI analysis of 400,000+ Reddit posts documenting real-world side effects and patient experiences with GLP-1 programs
Published by the PEPVi editorial team. Read our editorial standards.